Unrecognized Myasthenia Gravis Presenting as Prolonged Neuromuscular Blockade: A Case Report
Abstract
Background. Undiagnosed neuromuscular disease can present unexpectedly during anesthesia. We report prolonged neuromuscular blockade revealing previously unrecognized myasthenia gravis.
Methods. A 43-year-old woman underwent elective laparoscopic cholecystectomy. Standard-dose rocuronium was administered.
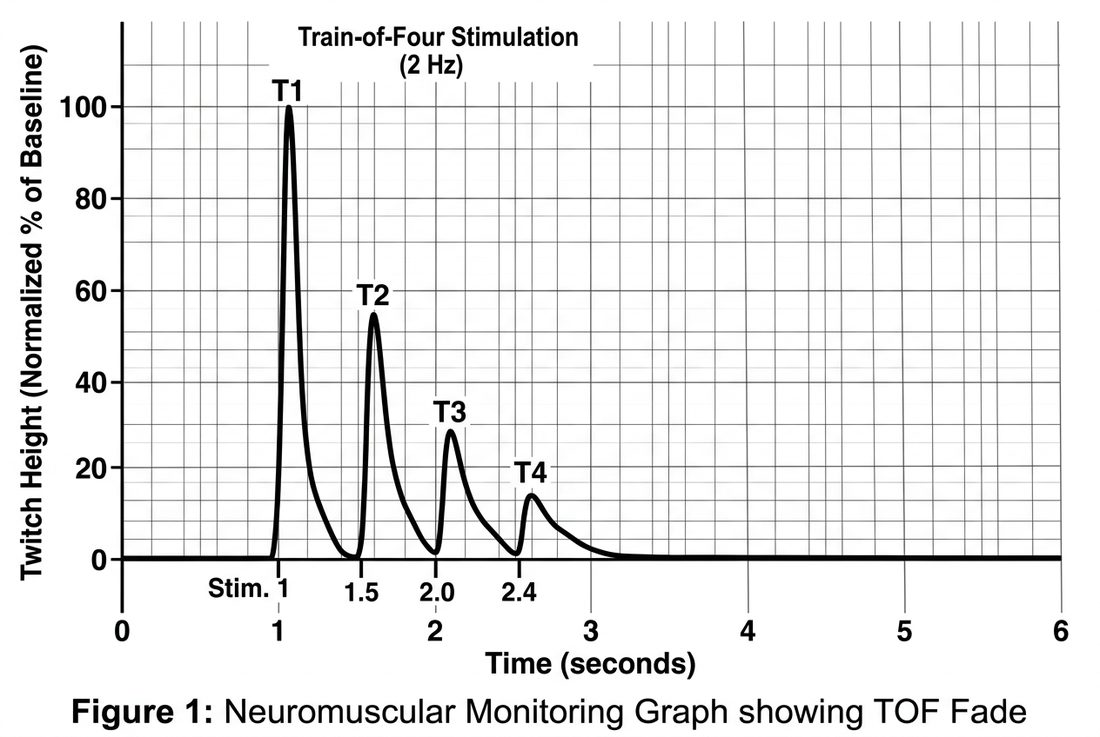
Results. Recovery of neuromuscular function was markedly delayed despite reversal. Postoperative work-up demonstrated positive acetylcholine receptor antibodies and a decremental response on repetitive nerve stimulation, confirming myasthenia gravis.
Conclusions. Anesthesiologists should consider occult neuromuscular disease when recovery from non-depolarizing agents is unexpectedly prolonged. Quantitative neuromuscular monitoring is essential.
Keywords
INTRODUCTION
METHODS
RESULTS
DISCUSSION
CONCLUSION
article.figures
References
- Blichfeldt-Lauridsen L, Hansen BD. Anesthesia and myasthenia gravis. Acta Anaesthesiol Scand. 2012;56(1):17-22.
- Gilhus NE. Myasthenia gravis. N Engl J Med. 2016;375(26):2570-2581.
- Brull SJ, Kopman AF. Current status of neuromuscular reversal and monitoring. Anesthesiology. 2017;126(1):173-190.
- Naguib M, Brull SJ, Kopman AF, et al. Consensus statement on perioperative use of neuromuscular monitoring. Anesth Analg. 2018;127(1):71-80.
- Sungur Z, Senturk M. Anaesthesia for thymectomy in myasthenia gravis. Curr Opin Anaesthesiol. 2016;29(1):14-19.