Case Report
Thrombotic Thrombocytopenic Purpura as the Initial Manifestation of Systemic Lupus Erythematosus: A Case Report
Isabela Cardoso, MD*; Ahmed Farouk, MD; Marta Kowalski, MD
Vol. 1, Issue 2 · April 02, 2026
Abstract
Background. Thrombotic thrombocytopenic purpura (TTP) rarely heralds systemic lupus erythematosus (SLE). We report such a presentation.
Methods. A 29-year-old woman presented with microangiopathic hemolytic anemia, thrombocytopenia and neurologic symptoms.
Results. ADAMTS13 activity was severely reduced. Autoimmune work-up revealed positive antinuclear and anti-dsDNA antibodies with low complement, consistent with SLE. She responded to plasma exchange and immunosuppression.
Conclusions. TTP may be the first manifestation of SLE. Prompt recognition and plasma exchange are life-saving; autoimmune screening should follow.
Keywords
thrombotic thrombocytopenic purpurasystemic lupus erythematosusADAMTS13plasma exchangemicroangiopathy
INTRODUCTION
TTP is a thrombotic microangiopathy caused by severe deficiency of ADAMTS13. Association with autoimmune disease is recognized, but TTP as the presenting feature of SLE is uncommon. Severe deficiency of ADAMTS13 leads to accumulation of ultralarge von Willebrand factor multimers and platelet-rich microthrombi within the microcirculation. When TTP arises in the context of autoimmunity, distinguishing it from other thrombotic microangiopathies is critical because delayed plasma exchange is associated with high mortality.
METHODS
We describe clinical presentation, laboratory findings, treatment and outcome.
RESULTS
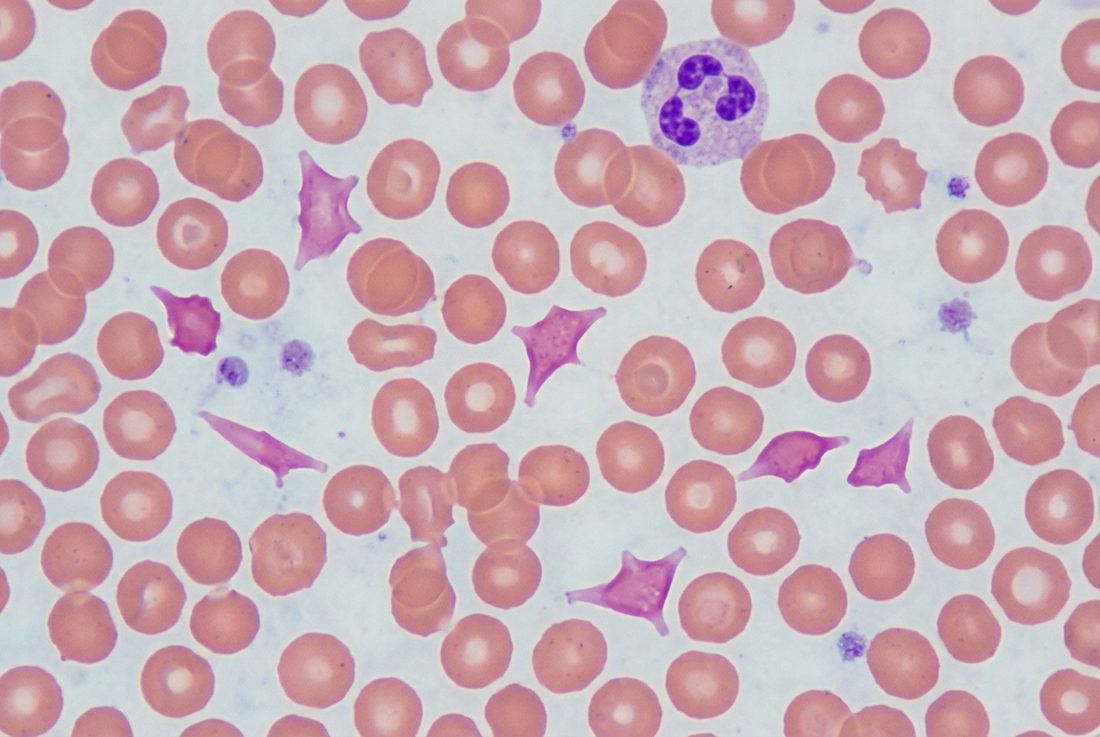
The pentad was incompletely expressed. Blood film showed schistocytes; LDH was markedly elevated. ADAMTS13 activity was <10%. Daily plasma exchange, corticosteroids and rituximab produced remission over two weeks.
DISCUSSION
The overlap between TTP and SLE reflects shared autoimmune mechanisms. Distinguishing TTP from lupus nephritis-associated microangiopathy is essential because treatment differs. Early plasma exchange remains the cornerstone. The coexistence of TTP and SLE may reflect a shared loss of immune tolerance, with autoantibodies directed against ADAMTS13. Rituximab is increasingly used to reduce relapse in immune-mediated TTP. Long-term rheumatologic follow-up is warranted because the hematologic presentation may precede other manifestations of lupus.
CONCLUSION
Clinicians should screen for SLE in patients presenting with acquired TTP, as concurrent immunosuppression may improve outcomes.
article.figures
References
- Joly BS, Coppo P, Veyradier A. Thrombotic thrombocytopenic purpura. Blood. 2017;129(21):2836-2846.
- Scully M, Cataland S, Coppo P, et al. Consensus on the standardization of terminology in TTP. J Thromb Haemost. 2017;15(2):312-322.
- Letchumanan P, Ng HJ, Lee LH, et al. TTP and SLE. Rheumatology. 2009;48(4):399-403.
- Kello N, Khoury LE, Marder G, et al. Secondary thrombotic microangiopathy in SLE. Semin Arthritis Rheum. 2019;49(1):74-83.