Original Research
Predictors of Readmission in Infants Hospitalized with Acute Bronchiolitis: A Multicenter Cohort
Lucia Moreno, MD*; Tomas Ibarra, MD; Aisha Rahman, MD
Vol. 1, Issue 1 · April 11, 2026
Abstract
Background. Acute bronchiolitis is the leading cause of infant hospitalization. Identifying readmission risk supports safe discharge planning.
Methods. Multicenter retrospective cohort of 738 infants <12 months hospitalized with bronchiolitis. 30-day respiratory readmission was the outcome. Multivariable logistic regression was used.
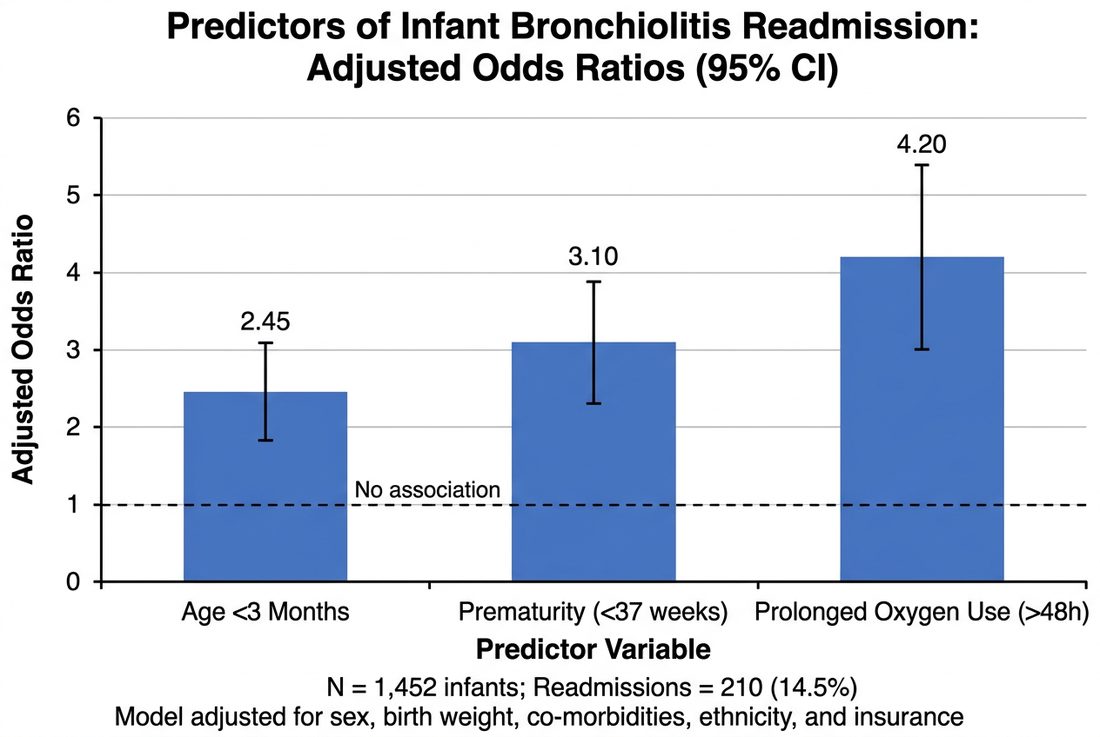
Results. Readmission occurred in 71 infants (9.6%). Independent predictors were age <3 months (OR 2.44), prematurity <37 weeks (OR 2.02), and need for supplemental oxygen >48 hours during index admission (OR 1.88).
Conclusions. Younger and premature infants and those with prolonged oxygen needs are at higher readmission risk and may benefit from closer follow-up.
Keywords
bronchiolitisinfantsreadmissionrespiratory syncytial viruspediatrics
INTRODUCTION
Most infants with bronchiolitis recover with supportive care, but a subset deteriorates after discharge and requires readmission. Predictive factors help clinicians tailor discharge criteria and follow-up. Bronchiolitis imposes a substantial seasonal burden on pediatric services. While guidelines emphasize supportive care, clinicians frequently face uncertainty at discharge, particularly for the youngest infants in whom deterioration can be rapid and difficult to predict.
METHODS
Infants under one year hospitalized with a first episode of clinically diagnosed bronchiolitis at four centers over two seasons were included. Demographic, clinical and treatment variables were extracted. Thirty-day respiratory readmission was modeled with multivariable logistic regression.
RESULTS
Among 738 infants, 71 (9.6%) were readmitted within 30 days. Median time to readmission was 6 days. Age <3 months, prematurity and prolonged oxygen requirement were independently associated with readmission, while nebulized therapies were not. Most readmissions occurred within the first week after discharge and were managed without intensive care. Respiratory syncytial virus was the predominant identified pathogen among tested infants.
DISCUSSION
The identified factors reflect limited physiologic reserve in the youngest and preterm infants. The lack of association with bronchodilators is consistent with guideline recommendations against their routine use. Retrospective ascertainment is a limitation. Discharge pathways that incorporate age, gestational history and the duration of supplemental oxygen may help target early follow-up to the infants most likely to benefit. Educating caregivers about warning signs and ensuring accessible review appointments are simple, low-cost measures that could reduce avoidable readmission.
CONCLUSION
Simple clinical variables predict bronchiolitis readmission and can inform discharge and follow-up decisions.
article.figures
References
- Ralston SL, Lieberthal AS, Meissner HC, et al. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics. 2014;134(5):e1474-e1502.
- Florin TA, Plint AC, Zorc JJ. Viral bronchiolitis. Lancet. 2017;389(10065):211-224.
- Hasegawa K, Pate BM, Mansbach JM, et al. Risk factors for requiring intensive care among children with bronchiolitis. Acad Pediatr. 2015;15(1):77-81.
- Pelletier AJ, Mansbach JM, Camargo CA. Direct medical cost of bronchiolitis hospitalizations. Pediatrics. 2006;118(6):2418-2423.