Cholestatic Liver Dysfunction As A Predictor Of Severity In Leptospirosis: Role Of Direct Bilirubin And Development Of A Hepatic Score
Blanca Esthela Melendez Acosta, Resident*; Brandon Javier Uriarte Zamora, PA; Andrea Carolina Salas Puente, Resident; Eduardo Lopez Diaz, Resident; Jose Alejandro Gomez, PA; Edgar Saldaña Rocha, PA; Andrea Guadalupe Zambrano Leon, PA; Pablo Maggiani Aguilera, MBBS
July 13, 2026
Abstract
Introduction and objectives:
Leptospirosis is a worldwide zoonosis ranging from mild illness to severe multiorgan involvement. Its hepatic manifestation typically presents with disproportionate conjugated hyperbilirubinemia, whose prognostic value remains poorly explored. This study aimed to evaluate the association between direct bilirubin and adverse clinical outcomes, as well as to develop a simple hepatic score for early risk stratification.
Material and methods:
An observational, analytical, and prospective study was conducted in 73 adults with MAT confirmed leptospirosis, hospitalized between March 2024 and January 2026. A composite outcome was assessed (in-hospital death, acute kidney injury, septic shock, or hospital stay longer than 7 days). A hepatic score was developed through logistic regression including the variables albumin <3.5 g/dL, direct bilirubin ≥8 mg/dL, and INR >1.5. Discriminative capacity was evaluated using ROC curves.
Results:
A total of 58 patients (79.45%) presented the composite outcome. Direct bilirubin was independently associated with the composite outcome (OR 1.15; 95%CI 1.01-1.41). The developed hepatic score demonstrated a robust association with the composite outcome (OR 3.42; 95%CI 1.54-8.60), tripling the risk with each additional point, with an AUC of 0.73, sensitivity of 78.9%, and specificity of 60%.
Conclusions:
Direct bilirubin represents a relevant severity marker in leptospirosis, enabling the identification of patients at high risk of adverse outcomes. Its combination with INR and hypoalbuminemia allowed the development of a hepatic score potentially useful for risk stratification and therapeutic decision-making in endemic regions.
Keywords
Leptospirosis; Direct bilirubin; Cholestasis; Liver dysfunction; Prognosis.
INTRODUCTION
Leptospirosis is a globally distributed zoonosis that represents a major public health problem, particularly in tropical and subtropical regions, where environmental factors such as humidity, flooding, and exposure to contaminated water favor transmission1,2. Clinically, the disease spans a broad spectrum, ranging from mild, self-limited forms to severe disease with multiorgan involvement, including kidney failure, pulmonary hemorrhage, and hepatic dysfunction1,3. In this context, early identification of patients at high risk of adverse outcomes remains a relevant clinical challenge, particularly in resource-limited settings.
Hepatic involvement in leptospirosis is characterized by a predominantly cholestatic pattern, with conjugated hyperbilirubinemia and relatively modest elevations in transaminases, suggesting a pathophysiologic mechanism distinct from that of other acute liver diseases2,4. This phenomenon has been associated with impaired bile transport, endothelial dysfunction, and a systemic inflammatory response rather than extensive hepatocellular necrosis4,5. Several studies have shown that hyperbilirubinemia is associated with greater clinical severity and worse prognosis; however, most studies have focused on total bilirubin, with limited differentiation of bilirubin fractions and little exploration of direct bilirubin as a specific prognostic marker3,6. Furthermore, assessment of hepatic dysfunction in leptospirosis may benefit from integrating parameters that reflect different pathophysiologic components of liver injury1,2. Direct bilirubin is a marker of the characteristic cholestatic pattern of this disease, which is associated with impaired bile transport, endothelial dysfunction, and a systemic inflammatory response2. In contrast, serum albumin and the international normalized ratio (INR) are indicators of hepatic synthetic function and systemic disease severity, reflecting abnormalities in protein and coagulation factor synthesis7. Because hepatic involvement in leptospirosis typically manifests as functional dysfunction rather than extensive hepatocellular necrosis, the combination of direct bilirubin, albumin, and INR may provide a comprehensive, accessible, and clinically useful prognostic approach for early risk stratification. Although hepatic dysfunction is part of the systemic involvement of leptospirosis, its integration into risk-stratification tools applicable to clinical practice remains limited1,6. Existing scores focus primarily on overall organ dysfunction without specifically considering the prognostic value of readily available hepatic parameters7,8. Therefore, there remains a need to identify simple, reproducible, and clinically useful markers that can improve prognostic assessment. Direct bilirubin may represent a relevant indicator not only of hepatic dysfunction but also of underlying systemic disease severity.
Therefore, this study aimed to evaluate the association between hepatic dysfunction, with emphasis on direct bilirubin, and clinical severity in patients with leptospirosis, as well as to develop a hepatic score based on routine laboratory parameters to improve risk stratification in this population.
METHODS
Study design and population
An observational, analytical, prospective cohort study was conducted in adult patients diagnosed with leptospirosis who were hospitalized in the Department of Internal Medicine at the General Hospital of Mazatlán, Sinaloa, Mexico, from March 2024 to January 2026. The composite endpoint comprised death, acute kidney injury, septic shock, or prolonged hospital stay. Hepatic parameters, including direct bilirubin, albumin, and INR, were analyzed, and a hepatic score was constructed on the basis of these variables. Direct bilirubin, serum albumin, and INR were selected because they assess different components of leptospirosis-associated hepatic dysfunction. Direct bilirubin reflects the characteristic cholestatic pattern, whereas albumin and INR are markers of hepatic synthetic function and systemic disease severity. In addition, these are routine, accessible, and reproducible laboratory parameters with potential utility for prognostic stratification in leptospirosis2,7. Discriminative ability was assessed using receiver operating characteristic (ROC) curves. The study population included all patient records meeting the inclusion criteria and with a confirmatory diagnosis by the microscopic agglutination test (MAT). Patients younger than 18 years, those with incomplete records, unconfirmed diagnoses, pre-existing chronic liver disease, documented biliary obstruction, or advanced chronic kidney disease, and records that did not permit adequate analysis of the primary variables were excluded.
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational cohort studies were followed9.
Data collection
Data were obtained from the institutional electronic medical record. Samples were collected at hospital admission, ensuring simultaneous measurements by the central laboratory under established quality standards. Informed consent was obtained in accordance with local regulations, and anonymity was ensured through coding and restricted data access.
Statistical analysis
Statistical analysis was performed using a binary logistic regression model to evaluate the association between hepatic dysfunction and clinical outcomes in patients with leptospirosis. The dependent variable was a composite adverse outcome defined as death, acute kidney injury (increase in serum creatinine of ≥0.3 mg/dL within 48 hours or ≥1.5 times baseline within 7 days10), septic shock, or prolonged hospital stay >7 days. The main independent variables were direct bilirubin, serum albumin, and INR at admission, along with clinically relevant adjustment variables. A descriptive analysis of the study population was performed, followed by bivariate analysis to identify significant associations using parametric or nonparametric tests according to data distribution. Variables with statistical significance or clinical relevance were entered into a multivariable model, and odds ratios (ORs) with 95% confidence intervals (CIs) were estimated. Model goodness-of-fit was assessed using the Hosmer-Lemeshow test. A hepatic score was then developed from the beta coefficients of the final model. Its discriminative ability was evaluated using ROC curves, with calculation of the area under the curve (AUC), sensitivity, specificity, positive predictive value, and negative predictive value. Analyses were performed using RStudio version 4.3.2.
Bias
To mitigate potential sources of bias, the study implemented several methodological and analytical strategies. First, to control measurement and information bias, clinical sample collection was standardized strictly at the time of hospital admission, and all samples were processed simultaneously by the central laboratory under quality standards. To reduce confounding related to underlying conditions, strict exclusion criteria were applied to remove patients with pre-existing chronic liver disease, documented biliary obstruction, or advanced chronic kidney disease. Diagnostic homogeneity was further ensured by requiring confirmation of all cases with the MAT. Finally, at the analytical level, a multivariable logistic regression model incorporating clinically relevant adjustment variables was used to control for potential confounders and estimate the independent contribution of hepatic markers to prognosis.
Ethical considerations
The protocol was approved by the Research Ethics Committee of the participating hospital (approval number CEI-2026-08). Data confidentiality was ensured in accordance with the Mexican General Health Law governing research involving human participants. The study was conducted in compliance with the ethical principles of the Declaration of Helsinki.
RESULTS
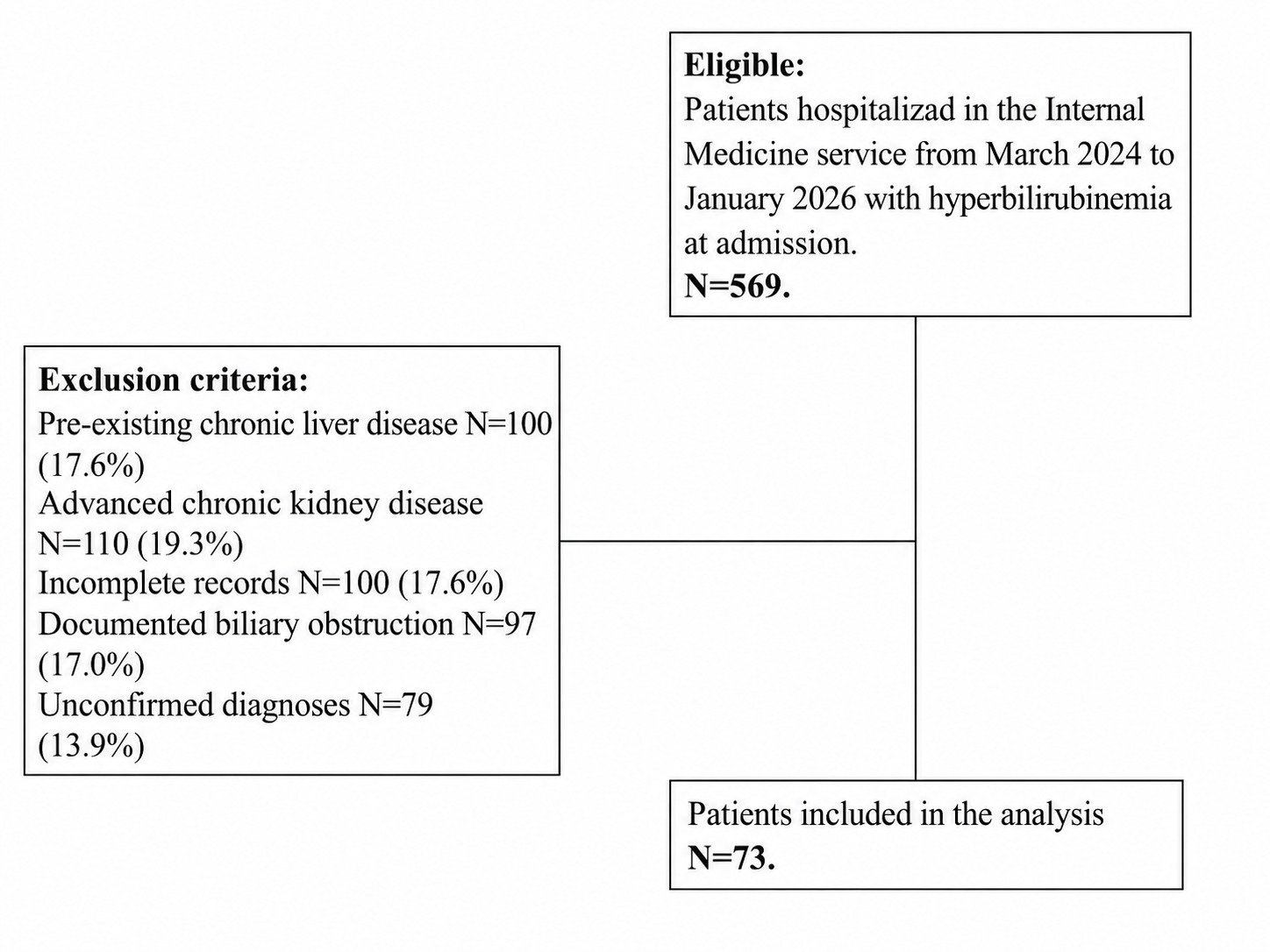
Of 569 patients assessed with hyperbilirubinemia at admission, 496 were excluded because they met exclusion criteria (incomplete records, unconfirmed diagnoses, pre-existing chronic liver disease, documented biliary obstruction, advanced chronic kidney disease, or lack of informed consent), leaving 73 patients for analysis (Figure 1). The mean age was 43.0 ± 19.1 years, and 63% of patients were male. The most frequent comorbidities were substance use (30.6%), type 2 diabetes mellitus (19.2%), and hypertension (12.3%). Initial laboratory testing showed a profile compatible with severe systemic illness, characterized by moderate anemia, leukocytosis, relative thrombocytopenia, renal dysfunction with urea 111.7 ± 90.6 mg/dL and creatinine 2.75 ± 2.54 mg/dL, and marked hyperbilirubinemia with predominance of the direct fraction (69.9 ± 15.9%). The predominant hepatic pattern was cholestatic (86.3%), with marked elevations in alkaline phosphatase and transaminases. Regarding clinical outcomes, acute kidney injury (increase in serum creatinine of ≥0.3 mg/dL within 48 hours or ≥1.5 times baseline within 7 days) occurred in 38 patients (52.05%), prolonged hospital stay (≥7 days) in 38 patients (52.05%), septic shock in 10 patients (13.7%), and in-hospital death in 17 patients (23.3%). The composite endpoint, defined as the occurrence of death, acute kidney injury, septic shock, or prolonged hospital stay, occurred in 58 patients (79.45%) (Table 1).
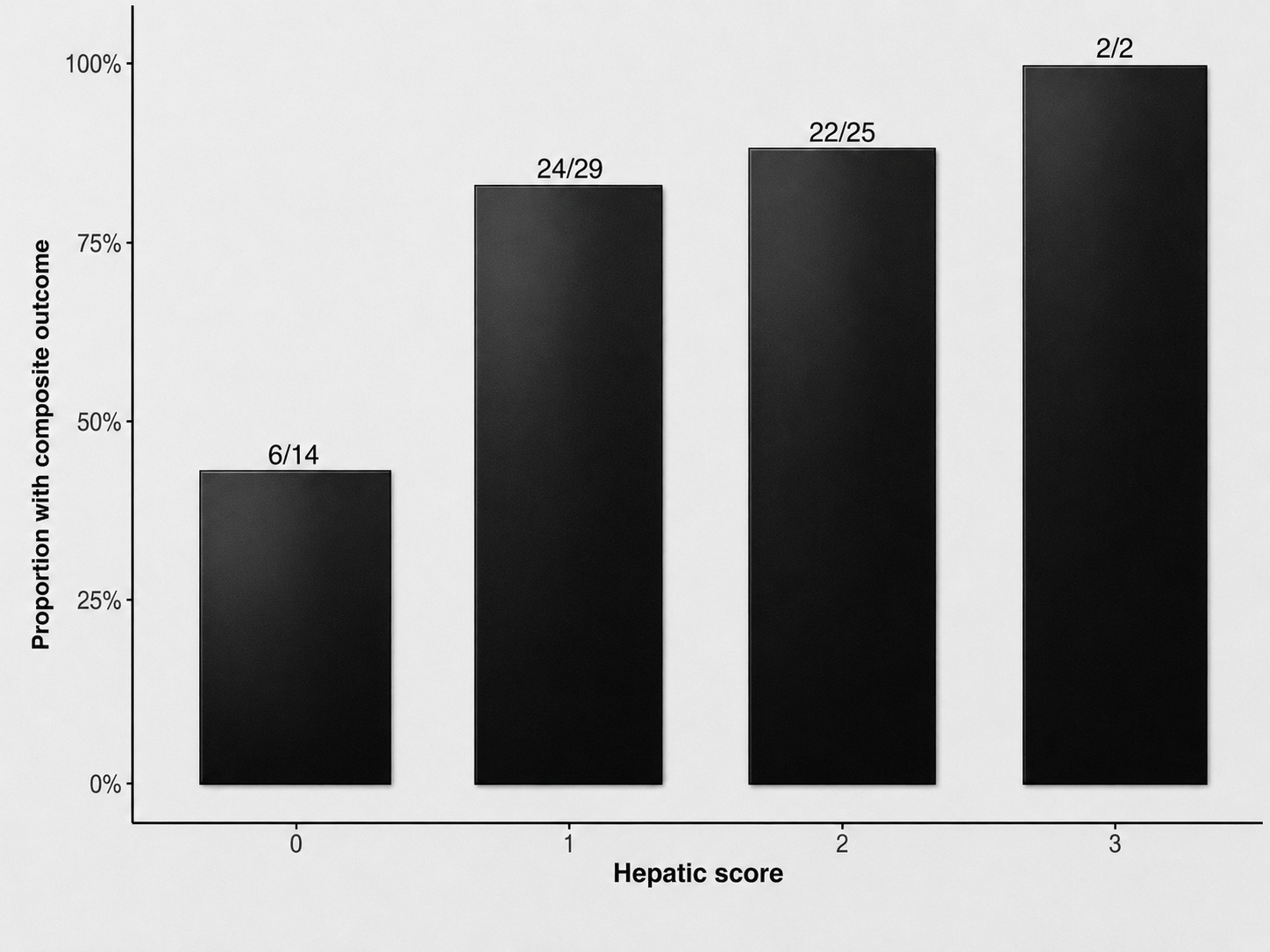
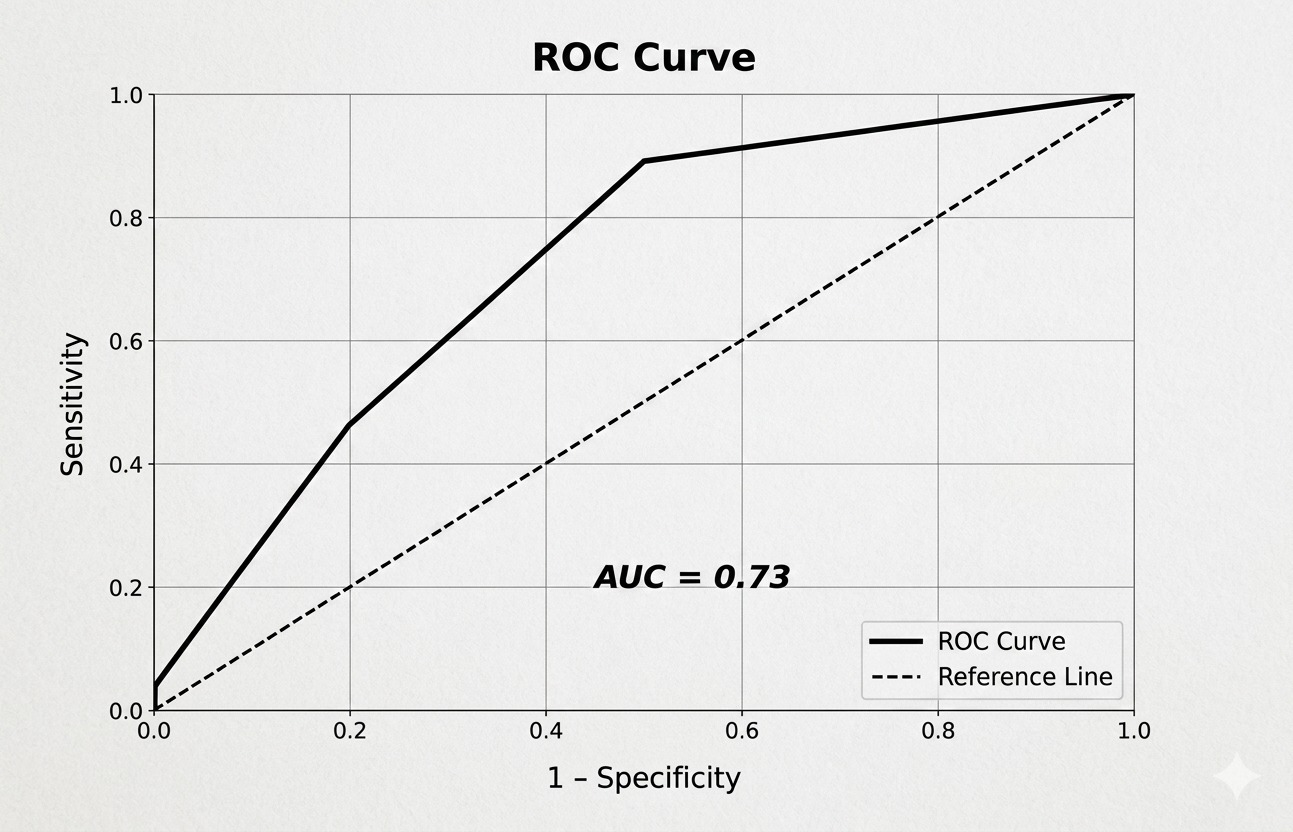
Direct bilirubin was significantly associated with the composite endpoint. In univariable analysis, each 1 mg/dL increase in direct bilirubin was associated with higher odds of an adverse outcome (OR 1.15; 95% CI 1.01-1.41). When direct bilirubin was categorized into quartiles, a progressive increase in the frequency of the composite endpoint was observed. The highest quartile (≥8 mg/dL) had a 100% composite endpoint rate. A hepatic score was constructed using three variables: albumin <3.5 g/dL, direct bilirubin ≥8 mg/dL, and INR >1.5. The score distribution was as follows: 0 points in 14 patients (19%), 1 point in 29 patients (40%), 2 points in 25 patients (34%), and 3 points in 2 patients (3%). The score showed a graded pattern, with a progressive increase in the frequency of the composite endpoint as the score increased: approximately 43% among patients with a score of 0, 83%-88% among those with scores of 1-2, and 100% among those with a score of 3 (Figure 2). In logistic regression analysis, the hepatic score was significantly associated with the composite endpoint (OR 3.42; 95% CI 1.54-8.60), indicating that each 1-point increase in the score was associated with more than a threefold increase in the odds of an adverse outcome. The hepatic score showed moderate discriminative ability, with an AUC of 0.73, sensitivity of 78.9%, specificity of 60%, PPV of 70%, and NPV of 65% (Figure 3).
DISCUSSION
In this study, we evaluated the role of hepatic dysfunction markers in hospitalized patients with leptospirosis and found that direct bilirubin at admission was significantly associated with clinical severity, defined by a composite endpoint of adverse events. This association was consistent when direct bilirubin was analyzed both as a continuous variable and after categorization, demonstrating a progressive risk gradient. Taken together, these results support direct bilirubin as an early marker of severe systemic disease.
From a hepatology perspective, our findings reinforce the concept of a cholestatic phenotype in leptospirosis, characterized by disproportionate conjugated hyperbilirubinemia relative to comparatively modest elevations in aminotransferases4,6. This pattern has been described as a distinctive feature of the disease and suggests a predominant pathophysiologic mechanism of functional hepatobiliary dysfunction rather than structural hepatocellular injury4,5. This abnormality has been proposed to reflect the interplay of endothelial dysfunction, microcirculatory disturbances, and systemic inflammatory mechanisms affecting bile transport4,6. In this context, elevated direct bilirubin may be interpreted as an indirect marker of the magnitude of systemic involvement.
Recent evidence from Wickramasinghe et al.11 and Griebsch et al.12 has further highlighted the relevance of this cholestatic pattern in leptospirosis, suggesting that conjugated hyperbilirubinemia may reflect systemic disease severity rather than isolated liver injury, thereby reinforcing its role as a prognostic biomarker.
Similarly, Marinho et al.13 and Smith et al.14 have reported that biomarkers derived from routine laboratory parameters may improve early risk stratification, supporting the development of simplified clinical tools in this setting13,14.
One of the most relevant findings of our study was the identification of a direct bilirubin cutoff of ≥8 mg/dL, above which the composite endpoint was markedly concentrated. Although the association between hyperbilirubinemia and severity has previously been documented in leptospirosis, most studies have focused on total bilirubin, with limited differentiation of its fractions7,8,15. In this regard, our results provide additional evidence suggesting a clinically relevant threshold for direct bilirubin. However, given the sample size and the occurrence of complete separation at the highest values, this finding should be interpreted cautiously and considered hypothesis-generating.
The development of a hepatic score based on direct bilirubin, albumin, and INR allowed integration of different dimensions of hepatic function and showed a significant association with the composite endpoint and a graded relationship with risk. This approach is consistent with strategies used in organ dysfunction scores such as SOFA16,17, which integrate multiple parameters to estimate clinical severity. From a clinical standpoint, the principal strength of this score lies in the simplicity and availability of its components, which may facilitate its use in resource-limited settings. However, its discriminative ability was moderate, and its clinical utility should be considered preliminary. Accordingly, the proposed score should be regarded as an exploratory derivation tool requiring internal and external validation before implementation in clinical practice.
This study has several important strengths. First, it specifically evaluates direct bilirubin as a marker of cholestatic hepatic dysfunction, an aspect that has been relatively underexplored in the literature, while providing an approach with strong pathophysiologic plausibility. Second, the consistency of the findings across different analytical approaches, together with the identification of a potentially clinically relevant cutoff, strengthens the robustness of the results. In addition, development of a hepatic score based on variables readily available at admission provides a potentially useful tool for clinical practice, particularly in resource-limited settings.
Several limitations should be acknowledged. The sample size was relatively small, which may have affected statistical power and the stability of the multivariable models. Nevertheless, this limitation should be interpreted within the epidemiologic context of leptospirosis, a disease with focal distribution whose incidence depends on environmental and seasonal factors. In this context, the inclusion of 73 hospitalized patients from an endemic region represents a clinically representative real-world cohort, particularly across the spectrum of moderate-to-severe disease, and is consistent with previous clinical series. In addition, the retrospective, single-center design introduces the possibility of selection bias and limits generalizability. Complete separation in some analyses precluded precise estimation of effect size using conventional methods, and the proposed hepatic score has not been externally validated; therefore, its utility should be considered preliminary. Overall, these findings should be considered hypothesis-generating and require confirmation in larger prospective studies with external validation.
CONCLUSION
Direct bilirubin is a relevant marker of severity in leptospirosis, particularly at elevated levels, because it enables identification of patients at high risk of adverse outcomes. In addition, combining elevated direct bilirubin with hepatic abnormalities such as increased INR and hypoalbuminemia enabled the development of a potentially useful hepatic score to improve risk stratification and support therapeutic decision-making, particularly in endemic regions where leptospirosis is a clinically important disease.
article.figures
Figure 1. Figure 1 Flowchart of the study population.Figure 2. Figure 2. Relationship between the hepatic score and the proportion of adverse outcomes. An increasing trend in the rate of adverse outcomes is observed as the hepatic score increases (values from 0 to 3). Numeric labels represent the number of events over the total number of patients evaluated at each score level.Figure 3. Figure 3. Receiver operating characteristic (ROC) curve of the hepatic score. The graph illustrates the model's discriminative ability for the composite endpoint, with an area under the curve (AUC) of 0.73. The solid line represents the score's performance compared with the reference line (dashed), at the cutoff corresponding to a sensitivity of 78.9% and specificity of 60%.
References
Bharti AR, Nally JE, Ricaldi JN, et al. Leptospirosis: a zoonotic disease of global importance. Lancet Infect Dis 2003;3:757-71.
Levett PN, Haake DA, Vinetz JM, et al. Leptospirosis. Clin Microbiol Rev 2001;14:296-326.
Haake DA, Levett PN, Bharti AR, et al. Leptospirosis in humans. Curr Top Microbiol Immunol 2015;387:65-97.
Yang CW, Bharti AR, Levett PN, et al. Leptospirosis renal disease: understanding the initiation by Toll-like receptors. Kidney Int 2007;72:918-25.
Andrade L, Daher EF, Seguro AC, et al. Leptospiral nephropathy. Semin Nephrol 2008;28:383-94.
Van Slambrouck CM, Salem F, Meehan SM, et al. Bile cast nephropathy is a common cause of acute kidney injury in severe liver dysfunction. Kidney Int 2013;84:192-7.
Daher EF, Zanetta DM, Cavalcante MB, et al. Risk factors for death and changing patterns in leptospirosis acute renal failure. Am J Trop Med Hyg 1999;61:630-4.
Doudier B, Garcia S, Quennee V, et al. Prognostic factors associated with severe leptospirosis. Clin Microbiol Infect 2006;12:299-300.
STROBE Initiative, Vandenbroucke JP, von Elm E, et al. STROBE Statement - Checklist of items that should be included in reports of observational studies. STROBE Initiative 2007. Available at: https://www.strobe-statement.org/
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group, Kellum JA, Lameire N, et al. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012;2:1-138.
Wickramasinghe M, Chandraratne A, Doluweera D, et al. Predictors of severe leptospirosis: a review. Eur J Med Res 2025;30:445. doi:10.1186/s40001-025-02518-2.
Griebsch C, Norris JM, Ward MP, et al. Emerging human leptospirosis: clinical and epidemiological insights. Sci One Health 2025;4:100126.
Marinho M, de Oliveira D, Monteiro DL, et al. Predictors of severe leptospirosis and mortality: a systematic review. Rev Inst Med Trop Sao Paulo 2021;63:e62.
Smith S, Kennedy BJ, Dermedgoglou A, et al. A simple score to predict severe leptospirosis. PLoS Negl Trop Dis 2019;13:e0007205.
Tubiana S, Mikulski M, Becam J, et al. Risk factors and predictors of severe leptospirosis in New Caledonia. PLoS Negl Trop Dis 2013;7:e1991.
Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med 1996;22:707-10.
Raith EP, Udy AA, Bailey M, et al. Prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA 2017;317:290-300.
How to cite this article
Blanca Melendez A., Brandon Uriarte Z., Andrea Salas P., et al. COLESTATIC LIVER DYSFUNCTION AS A PREDICTOR OF SEVERITY IN LEPTOSPIROSIS: ROLE OF DIRECT BILIRUBIN AND DEVELOPMENT OF A HEPATIC SCORE. Clin Surg Rev. 2026.