Original Research
Diagnostic Performance of Point-of-Care Ultrasound for Acute Dyspnea in the Emergency Department
Paula Navarro, MD*; Hassan Karim, MD; Bruno Ferreira, MD
Vol. 2, Issue 1 · June 22, 2026
Abstract
Background. Acute dyspnea is a common and diagnostically challenging emergency presentation. We evaluated point-of-care ultrasound (POCUS) for rapid etiologic diagnosis.
Methods. Prospective diagnostic study of 284 adults presenting with acute dyspnea. Integrated cardiopulmonary POCUS was compared with the final diagnosis adjudicated after full work-up.
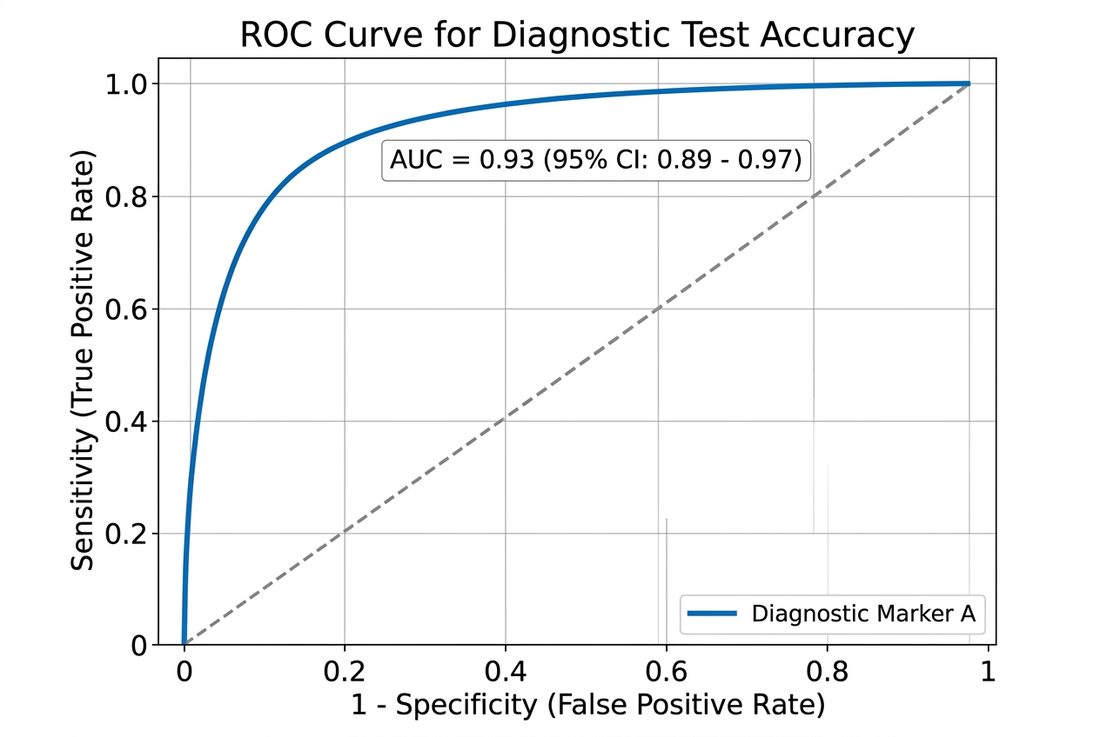
Results. POCUS had a sensitivity of 89.7% and specificity of 86.4% for acute decompensated heart failure, and reduced median time to correct diagnosis from 96 to 24 minutes.
Conclusions. Integrated POCUS improves diagnostic accuracy and accelerates decision-making in emergency patients with acute dyspnea.
Keywords
point-of-care ultrasoundacute dyspneaemergency departmentlung ultrasounddiagnostic accuracy
INTRODUCTION
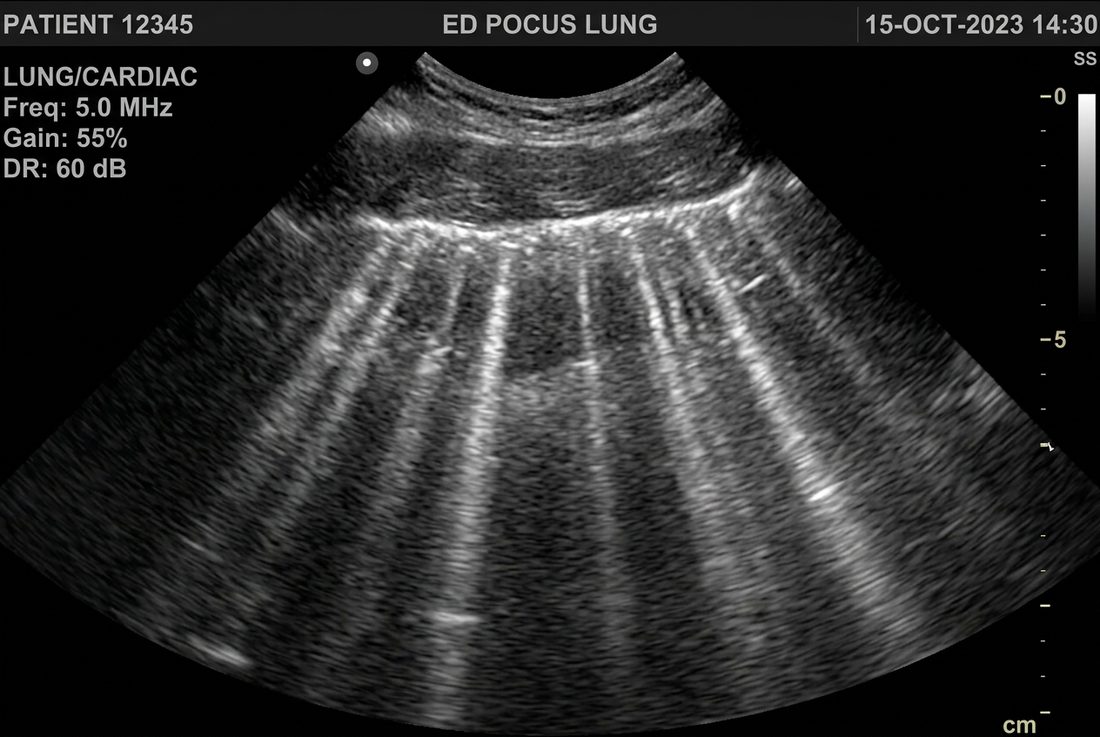
Distinguishing cardiac from pulmonary causes of acute dyspnea at the bedside is difficult but time-critical. POCUS integrates lung, cardiac and inferior vena cava assessment to narrow the differential rapidly. Undifferentiated dyspnea is one of the most common and highest-acuity presentations in emergency medicine, and misclassification carries real risk because treatments for the leading causes are frequently opposed. Point-of-care ultrasound brings imaging to the bedside and can be integrated seamlessly into the initial evaluation.
METHODS
Consecutive adults with undifferentiated acute dyspnea were prospectively enrolled. Treating emergency physicians performed a standardized POCUS protocol before laboratory and radiographic results. The reference standard was the discharge diagnosis adjudicated by two independent physicians.
RESULTS
Among 284 patients, POCUS showed high sensitivity and specificity for acute decompensated heart failure and pneumothorax, and shortened time to correct diagnosis. Diagnostic reclassification occurred in 21% of cases after POCUS. Inter-rater agreement for the key sonographic findings was substantial. The greatest incremental value of POCUS was observed in patients whose initial clinical impression was uncertain.
DISCUSSION
These results support integrating POCUS early in the evaluation of dyspnea. Operator training and image quality influence accuracy; the single-center setting may limit generalizability. Integrating lung, cardiac and inferior vena cava assessment allows the clinician to rapidly converge on the dominant physiology driving dyspnea. Structured training and quality assurance are essential to reproduce these results outside high-volume academic centers.
CONCLUSION
Early integrated POCUS enhances and accelerates the diagnosis of acute dyspnea in the emergency department.
article.figures
References
- Volpicelli G, Elbarbary M, Blaivas M, et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012;38(4):577-591.
- Zanobetti M, Scorpiniti M, Gigli C, et al. Point-of-care ultrasonography for evaluation of acute dyspnea in the ED. Chest. 2017;151(6):1295-1301.
- Pivetta E, Goffi A, Lupia E, et al. Lung ultrasound-implemented diagnosis of acute decompensated heart failure. Chest. 2015;148(1):202-210.