Original Research
Neutrophil-to-Lymphocyte Ratio and In-Hospital Mortality in Sepsis: A Retrospective Analysis
Camila Rojas, MD*; Kwame Mensah, MD; Elena Petrova, MD, PhD
Vol. 1, Issue 1 · March 24, 2026
Abstract
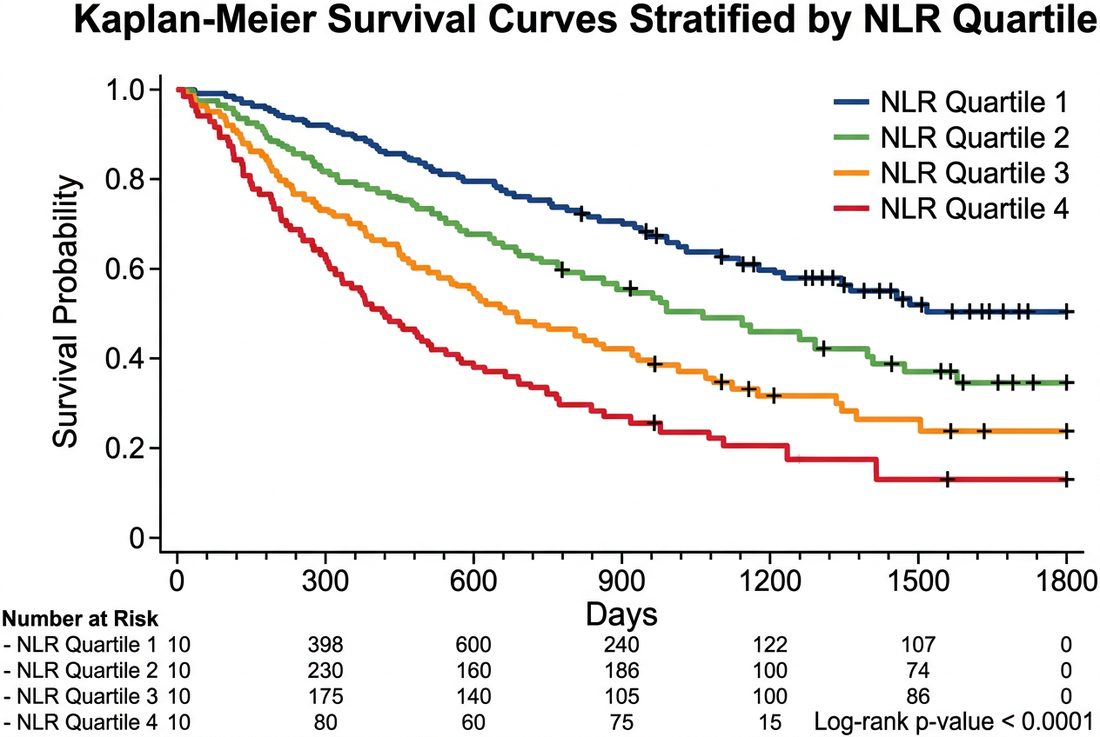
Background. The neutrophil-to-lymphocyte ratio (NLR) is an inexpensive marker of systemic inflammation. We evaluated its association with in-hospital mortality in sepsis.
Methods. Retrospective cohort of 596 adults admitted with sepsis. Admission NLR was analyzed in quartiles. Multivariable Cox regression adjusted for age, comorbidity and SOFA score.
Results. In-hospital mortality was 18.6%. Patients in the highest NLR quartile (>12.4) had significantly higher mortality than the lowest quartile (adjusted HR 2.08, 95% CI 1.31-3.30). NLR added incremental discrimination to the SOFA score.
Conclusions. Admission NLR is independently associated with in-hospital mortality in sepsis and may aid early risk stratification.
Keywords
sepsisneutrophil-to-lymphocyte ratiobiomarkermortalityprognosis
INTRODUCTION
Sepsis remains a leading cause of hospital death. Simple, widely available biomarkers that improve early prognostication are valuable, particularly in resource-limited settings. The NLR reflects the balance between innate activation and adaptive suppression. Systemic inflammation in sepsis is characterized by neutrophilia driven by demargination and delayed apoptosis, together with stress-induced and apoptosis-mediated lymphopenia. The NLR captures both arms of this dysregulated response in a single, inexpensive index derived from the routine complete blood count.
METHODS
We reviewed consecutive adult admissions meeting Sepsis-3 criteria over three years. Complete blood counts at admission were used to calculate NLR. Patients were grouped by quartile. Cox proportional-hazards models estimated the association with in-hospital mortality.
RESULTS
Among 596 patients, 111 died in hospital. Mortality rose across NLR quartiles from 9.4% to 29.1%. After adjustment, the highest quartile retained a two-fold hazard. Adding NLR to SOFA modestly improved the c-statistic. The association between NLR and mortality persisted across predefined subgroups, including patients with and without a documented microbiological source. Sensitivity analyses excluding patients with hematologic malignancy did not materially change the estimates.
DISCUSSION
The findings are consistent with prior reports linking lymphopenia and neutrophilia to poor sepsis outcomes. As a routine, low-cost parameter, NLR is attractive for triage. Retrospective design and single-center data limit causal inference. As a universally available parameter, NLR is particularly appealing for triage in settings where advanced biomarkers are inaccessible. It should complement rather than replace validated severity scores. Prospective multicenter validation and evaluation of serial NLR trajectories would strengthen its role in clinical decision-making.
CONCLUSION
NLR is a readily available prognostic marker in sepsis and complements established severity scores.
article.figures
References
- Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801-810.
- Liu Y, Zheng J, Zhang D, et al. Neutrophil-lymphocyte ratio and sepsis prognosis. Medicine. 2019;98(43):e17537.
- Hwang SY, Shin TG, Jo IJ, et al. Neutrophil-to-lymphocyte ratio as a prognostic marker in sepsis. Am J Emerg Med. 2017;35(2):234-239.
- Drewry AM, Samra N, Skrupky LP, et al. Persistent lymphopenia after sepsis. Shock. 2014;42(5):383-391.
- Zahorec R. Neutrophil-to-lymphocyte ratio, past, present and future. Bratisl Lek Listy. 2021;122(7):474-488.