Surgical Technique
Ultrasound-Guided Erector Spinae Plane Block for Thoracoabdominal Analgesia: A Step-by-Step Technique
Andres Villalba, MD*; Grace Tan, MD; Youssef Barakat, MD
Vol. 1, Issue 2 · March 15, 2026
Abstract
Background. The erector spinae plane (ESP) block is an interfascial regional technique providing thoracoabdominal analgesia. We describe a reproducible ultrasound-guided approach.
Methods. The technique is described from patient positioning and probe placement to needle trajectory, hydrodissection and catheter placement, with practical troubleshooting.
Results. Correct injection produces linear cephalocaudal spread deep to the erector spinae muscle at the target transverse process, with reliable multi-dermatomal coverage.
Conclusions. The ESP block is a straightforward, low-risk technique that can be incorporated into opioid-sparing multimodal analgesia protocols.
Keywords
erector spinae plane blockregional anesthesiaultrasoundanalgesiaopioid-sparing
INTRODUCTION
Adequate somatic analgesia after thoracic and upper abdominal surgery reduces pulmonary complications and opioid consumption. The ESP block deposits local anesthetic in the plane between the erector spinae muscle and the transverse process, achieving craniocaudal spread across multiple levels. Interfascial plane blocks have expanded the analgesic armamentarium by targeting the dorsal and ventral rami as local anesthetic spreads within a well-defined tissue plane. The ESP block is attractive because its landmarks are consistent and the injection point lies at a safe distance from the neuraxis and pleura.
METHODS
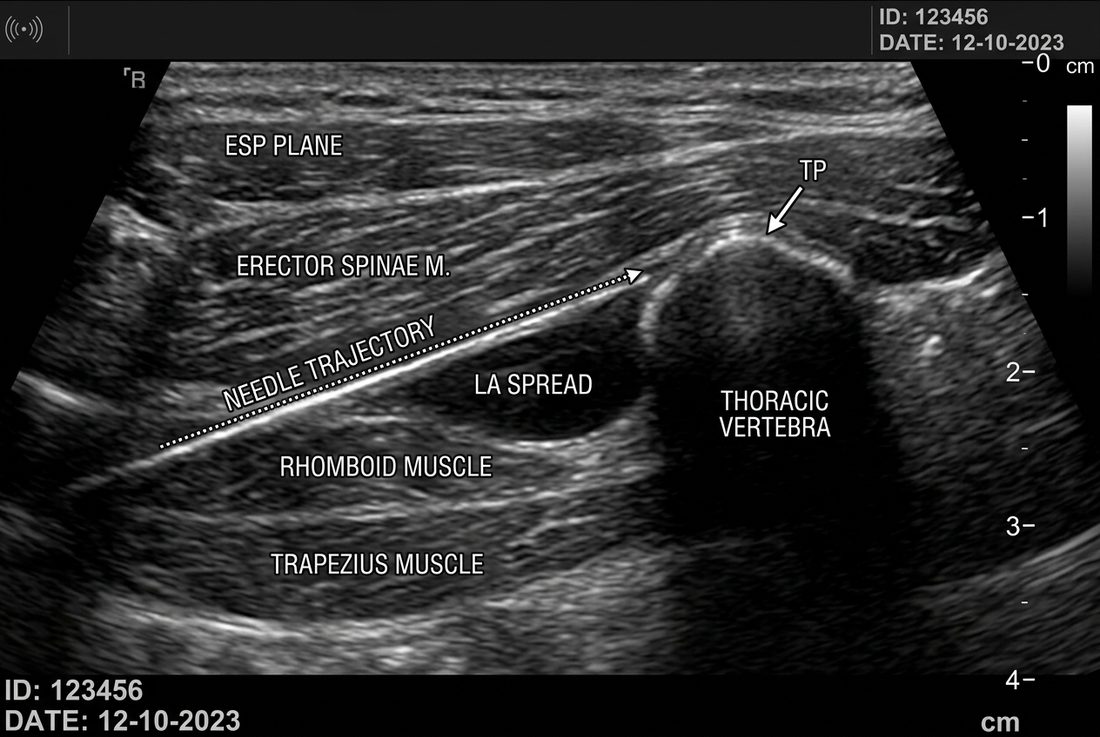
With the patient sitting or in lateral decubitus, a high-frequency linear probe is placed in a parasagittal orientation lateral to the spinous process at the target level. The transverse process is identified beneath the trapezius, rhomboid and erector spinae muscles. Using an in-plane cephalad-to-caudad approach, the needle tip is advanced to contact the transverse process. Hydrodissection confirms correct plane; local anesthetic is then injected. A catheter may be threaded for continuous analgesia.
RESULTS
Successful blockade is confirmed by visualized linear spread lifting the erector spinae muscle off the transverse process. Coverage typically extends several dermatomes above and below the injection level.
DISCUSSION
Because the injection site is distant from the pleura and neuraxis, the ESP block carries a favorable safety profile compared with paravertebral or neuraxial techniques. Careful ultrasound identification of the transverse process (a flat, bony acoustic shadow) distinguishes it from the rounded rib. Reported complications are rare and largely limited to those inherent to any regional technique. The block is well suited to enhanced-recovery pathways for thoracic, breast and upper abdominal surgery, and a catheter can extend analgesia into the postoperative period. Familiarity with sonographic identification of the transverse process is the principal determinant of success.
CONCLUSION
The ultrasound-guided ESP block is reproducible and safe, and is a valuable component of enhanced-recovery analgesic pathways.
article.figures
References
- Forero M, Adhikary SD, Lopez H, et al. The erector spinae plane block: a novel analgesic technique. Reg Anesth Pain Med. 2016;41(5):621-627.
- Chin KJ, El-Boghdadly K. Mechanisms of action of the erector spinae plane block. Can J Anaesth. 2021;68(3):387-408.
- Tulgar S, Ahiskalioglu A, De Cassai A, et al. Efficacy of ESP block. J Clin Anesth. 2019;57:3-4.
- Kot P, Rodriguez P, Granell M, et al. The erector spinae plane block: a narrative review. Korean J Anesthesiol. 2019;72(3):209-220.