Surgical Technique
Single-Incision Laparoscopic Cholecystectomy: Description of Technique and Initial Experience
Renata Lima, MD*; Ali Reza, MD; Katarzyna Wojcik, MD
Vol. 2, Issue 1 · June 04, 2026
Abstract
Background. Single-incision laparoscopic cholecystectomy (SILC) reduces the number of abdominal incisions. We describe our technique and early experience.
Methods. The technique covers port placement through a transumbilical multichannel device, exposure of Calot's triangle and the critical view of safety.
Results. SILC was completed successfully in the majority of selected patients, with attention to triangulation and ergonomic instrument crossing.
Conclusions. SILC is feasible and offers cosmetic benefit in selected patients when the critical view of safety is prioritized.
Keywords
single-incisionlaparoscopic cholecystectomycosmesisminimally invasivegallbladder
INTRODUCTION
Conventional laparoscopic cholecystectomy uses three to four ports. SILC consolidates access through a single umbilical incision, aiming to improve cosmesis and reduce port-site morbidity while preserving safety. Reducing the number and size of abdominal incisions has been a continuing goal of minimally invasive surgery. Single-incision laparoscopic cholecystectomy consolidates access through the umbilicus, offering improved cosmesis, but it introduces ergonomic challenges related to instrument crowding and loss of triangulation.
METHODS
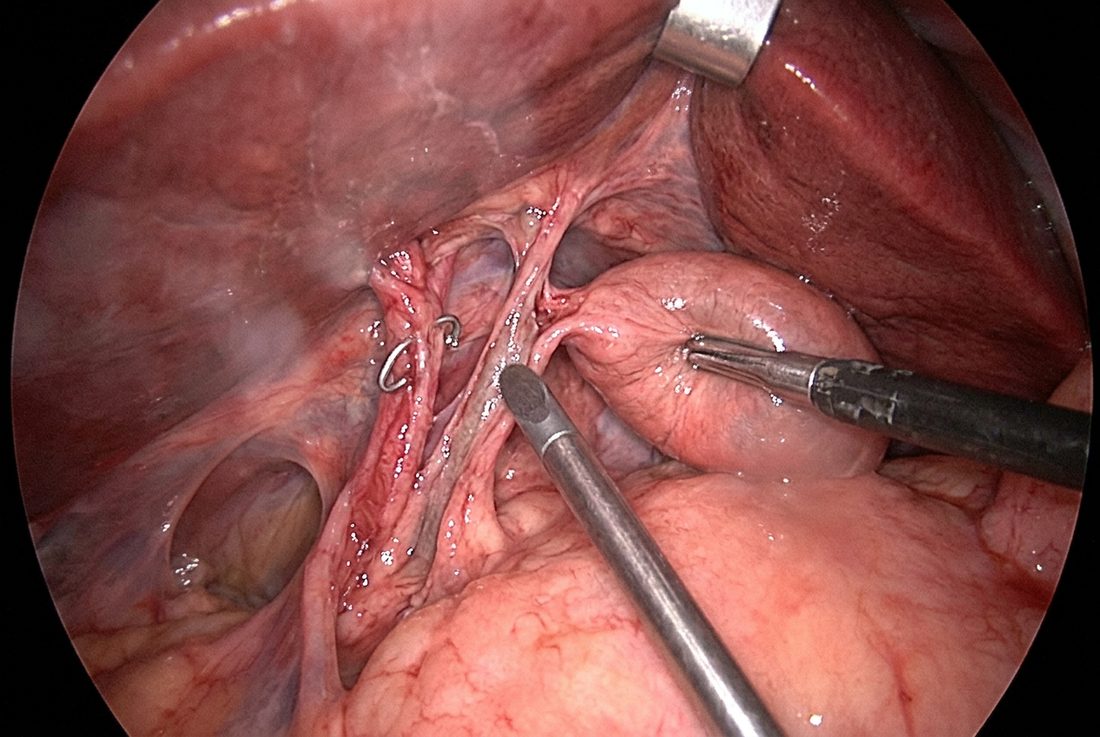
A 2-2.5 cm transumbilical incision accommodates a multichannel single-port device. A 5-mm 30-degree scope and articulating or crossed straight instruments are used. The fundus is retracted with a transabdominal suture. Dissection proceeds to obtain the critical view of safety before clipping and dividing the cystic duct and artery.
RESULTS
In the initial series, the procedure was completed without additional ports in most patients. Suture retraction improved exposure and offset the loss of triangulation inherent to single-port surgery.
DISCUSSION
SILC has a learning curve related to instrument clashing and limited triangulation. Strict adherence to the critical view of safety and a low threshold to add a port protect against biliary injury. Adherence to the critical view of safety is non-negotiable and is the single most important safeguard against bile duct injury. A low threshold to add an accessory port or convert to a conventional approach preserves safety while surgeons progress along the learning curve.
CONCLUSION
With appropriate patient selection and safety discipline, SILC is a reproducible, cosmetically favorable technique.
article.figures
References
- Strasberg SM, Brunt LM. Rationale and use of the critical view of safety in laparoscopic cholecystectomy. J Am Coll Surg. 2010;211(1):132-138.
- Hirano Y, Watanabe T, Uchida T, et al. Single-incision laparoscopic cholecystectomy: single institution experience. World J Gastroenterol. 2010;16(46):5851-5855.
- Trastulli S, Cirocchi R, Desiderio J, et al. Systematic review and meta-analysis of SILC versus conventional. Br J Surg. 2013;100(2):191-208.